Ceftin (Cefuroxime)

Dosages
Ceftin 125 mg
| Quantity | Price per tablet | You save | Total price | |
|---|---|---|---|---|
| 10 | $3.10 | - | $31.00 | |
| 30 | $3.07 | $1.00 | $92.00 | |
| 60 | $2.62 | $29.00 | $157.00 | |
| 90 | $2.64 | $41.00 | $238.00 |
Ceftin 250 mg
| Quantity | Price per tablet | You save | Total price | |
|---|---|---|---|---|
| 30 | $3.77 | - | $113.00 | |
| 60 | $2.98 | $47.00 | $179.00 | |
| 90 | $2.70 | $96.00 | $243.00 | |
| 120 | $2.57 | $144.00 | $308.00 |
Ceftin 500 mg
| Quantity | Price per tablet | You save | Total price | |
|---|---|---|---|---|
| 30 | $5.23 | - | $157.00 | |
| 60 | $3.93 | $78.00 | $236.00 | |
| 90 | $3.50 | $156.00 | $315.00 |
Payment & Shipping
Your order is carefully packed and ships within 24 hours. Here is what a typical package looks like.
Sized like a regular personal letter (9.4x4.3x0.3 inches), with no indication of what is inside.


| Shipping Method | Estimated delivery |
|---|---|
| Express Free for orders over $300.00 | Estimated delivery to the U.S.: 4-7 days |
| Standard Free for orders over $200.00 | Estimated delivery to the U.S.: 14-21 days |











Discount Coupons
- Independence Day - July 4, 2026 10% JULY410
- Labor Day - September 7, 2026 7% LABOR07
- Thanksgiving - November 26, 2026 9% THANKS09
Brand Names
| Country | Brand Names |
|---|---|
 Argentina Argentina | Ceflux Cefogram Cefurox Ligramex |
 Australia Australia | Zinnat |
 Belgium Belgium | Axetine Cefurim Doccefuro Kefurox Zinacef Zinnat |
 Brazil Brazil | Cefunorth Cefuran Keroxime Medcef Zinacef Zinnat |
 Canada Canada | Kefurox Zinacef |
 Czechia Czechia | Axetine Lifurox Xorimax Zinacef Zinnat Zinoxime |
 Denmark Denmark | Axacef Lifurox Zinacef Zinnat |
 Finland Finland | Kefurion Lifurox Zinacef Zinnat |
 France France | Cepazine Zinnat |
 Germany Germany | Cefu Cefudura Cefuhexal Cefurax Cefuro-Puren Cefurox Cefurox-Reu Cefurox-Wolff Elobact Zinacef Zinnat |
 Greece Greece | Anaptivan Cefoprim Cefur Cefuroprol Cerofene Ceruxim Cupax Ecoline Feacef Foucacillin Fredyr Furaxil Galemin Genephoxal Gonif Helatocil Interbion Lyprovir Medoxem Mevecan Mosalan Nelabocin Nipogalin Normafenac Receant Saxetil Sedopan Vekfazolin Yokel Zagorine Zetagal Zilisten Zinacef Zinadol |
 Hungary Hungary | Cefurin Ceroxim Cexim Xorim Xorimax Zinacef Zinnat |
 Italy Italy | Biociclin Biofurex Bioxima Cefamar Cefoprim Cefumax Cefur Cefurex Cefurin Colifossim Curoxim Deltacef Duxima Gibicef Ipacef Itorex Kefox Kesint Lafurex Lamposporin Medoxim Oraxim Polixima Supero Tilexim Ultroxim Zinnat Zinocep Zoref |
 Malaysia Malaysia | Altacef Ceflour Efurox Furoxime Xorimax Xylid Zinacef Zinnat Zocef |
 Mexico Mexico | Cefabiot Cefagen Cefuracet Cetoxil Froxal Fucerox Furobioxin Lemoxin Magnaspor Novador Ximaken Xorufec Zinnat |
 Netherlands Netherlands | Cefofix Zinacef Zinnat |
 New Zealand New Zealand | Axetine Zinacef Zinnat |
 Norway Norway | Lifurox Zinacef |
 Poland Poland | Biofuroksym Bioracef Ceroxim Novocef Oframax Plixym Tarsime Xorim Xorimax Zamur Zinacef Zinnat |
 Portugal Portugal | Antibioxime Axacef Cefaricida Cefofix Cefrix Condronac Curoxime Famicef Furaxetil Lusocef Pluscef Saracef Zipos Zoref |
 Spain Spain | Curoxima Lifurox Nivador Selan Zinnat |
 Sweden Sweden | Axacef Lifurox Zinacef Zinnat |
 Turkey Turkey | Aksef Cefatin Enfexia Multisef Oraceftin Sefaktil Sefuroks Zinnat |
 United States United States | Kefurox Zinacef |
| Manufacturer | Brand Names |
|---|---|
| Mankind Pharma | Cefakind |
Description
Ceftin is a prescription drug, an antibiotic used for the treatment of bacterial infections. It can be prescribed as monotherapy or as part of combination therapy. The active ingredient in the medication is cefuroxime axetil. It may interact with other medications and diseases, cause allergic reactions, and has a long list of possible side effects.

However, this antibiotic is useful for treating many types of bacterial infections.
In this article, you'll learn what cefuroxime axetil is used for, where to buy Ceftin online, what forms it comes in, how to store it, what cefuroxime side effects are, and more.
What Is Cefuroxime and What Is It Used For?
Cefuroxime (Ceftin) is a second-generation cephalosporin antibiotic. It's used for both mild symptoms and life-threatening forms of bacterial infections. It can also be prescribed by your doctor for uses not listed in the prescribing information.
The conditions treated by Ceftin include:
- Acute bacterial otitis media;
- Pharyngitis/tonsillitis;
- Acute bacterial maxillary sinusitis;
- Impetigo;
- Uncomplicated gonorrhea;
- Uncomplicated urinary tract infections;
- Bacterial infections associated with acute bronchitis;
- Acute bacterial exacerbations of chronic bronchitis;
- Uncomplicated skin and skin structure infections;
- Early Lyme disease.
All these conditions can be treated in adults and pediatric patients with this medicine. However, there are no clear clinical trial data on its use in children younger than 3 months old.

It's important to be sure that the infection is caused by susceptible bacteria if your doctor prescribes this medicine. Otherwise, inappropriate use may contribute to the development of drug-resistant bacteria.
What You Should Check Before Taking This Medicine
You should discuss use of this medicine with your doctor and tell them about your medical history and any drugs you take, including medicines you start or stop taking, as well as immunizations and vaccinations. It's also essential to disclose any allergies to penicillins, cefuroxime (in the form of axetil or otherwise), or other antibiotics.
Don't share this medication with other people even if they have similar symptoms.
Allergic Reaction to Similar Antibiotics
Do not use the medication if you're allergic to:
- Cefdinir (Omnicef);
- Cefprozil (Cefzil);
- Cephalexin (Keflex);
- Cefaclor (Raniclor);
- Cefadroxil (Duricef);
- Cefazolin (Ancef);
- Cefditoren (Spectracef);
- Cefpodoxime (Vantin);
- Ceftibuten (Cedax);
- Cephradine (Velosef).
It's recommended that you consult a pharmacist if you're not sure about the names of medicines you've taken before.
Conditions to Discuss Before Taking Ceftin
To be sure you can safely take cefuroxime axetil, tell your healthcare provider if you have any of the following, or symptoms that might indicate them:
- Penicillin allergy;
- Liver disease (may not process the medication properly and can cause buildup);
- Kidney disease (may cause buildup of medication in your body);
- Diabetes (the suspension contains about 3 g of sugar per teaspoon);
- Intestinal problems (colitis, even if resolved);
- Malnutrition;
- Anemia (cefuroxime may rarely cause certain types of anemia; if symptoms occur, contact your doctor immediately);
- Phenylketonuria (PKU) (the liquid form may contain phenylalanine);
- Any other bacterial infection (use of cefuroxime may allow other organisms to overgrow, causing yeast or other infections).
It's wise to tell your doctor about any other diseases you've had or allergies you've experienced, even if only once. Tell them if you're pregnant, planning to become pregnant, or breastfeeding, as these factors may affect the dosage of cefuroxime.
Do not take this drug without a prescription to treat conditions like the common cold or other non-bacterial infections. This may promote resistant bacteria, meaning the medication may not work when you need it in the future.
Medicine Description
Cefuroxime comes in three forms:
- Cefuroxime 250 mg tablets;
- Cefuroxime 500 mg tablets;
- Cefuroxime powder for oral suspension.
Ceftin 500 mg and 250 mg Tablets
The 500 mg tablets are:
- White;
- Capsule-shaped;
- Film-coated;
- Engraved with "GXEG2" on one side.
Aside from 500 mg of cefuroxime, they contain methylparaben, hydrogenated vegetable oil, titanium dioxide, and other ingredients.
The 250 mg tablets are:
- White;
- Capsule-shaped;
- Film-coated;
- Engraved with "GXES7" on one side.
Aside from 250 mg of cefuroxime, they contain methylparaben, hydrogenated vegetable oil, titanium dioxide, and other ingredients.
Ceftin for Oral Suspension
The suspension comes as dry granulated powder, white or pale yellow, with a tutti-frutti flavor. After mixing with water, each 5 mL contains 125 mg of cefuroxime, as well as sucrose, flavoring, xanthan gum, acesulfame potassium, aspartame, stearic acid, and polyvinylpyrrolidone.
Preparation and Administration of Ceftin for Oral Suspension
Prepare the suspension by:
- Shaking the bottle of powder to mix and loosen it;
- Opening the bottle and adding water as directed in the instructions;
- Closing the bottle;
- Turning the bottle upside down, then rocking and shaking the bottle until the water passes through the powder;
- Turning the bottle upright and shaking diagonally until the mixture is uniform.
Shake the mixture every time before use and close the bottle tightly after each use. Store it in the refrigerator at 36-46°F (2-8°C). If it is not finished within 10 days, discard the mixture and prepare a new suspension when needed.
How to Take Ceftin Tablets
How you take Ceftin depends on the condition being treated. Review the information below and read the medication guide before starting treatment.
Cefuroxime Dosage for Tablets
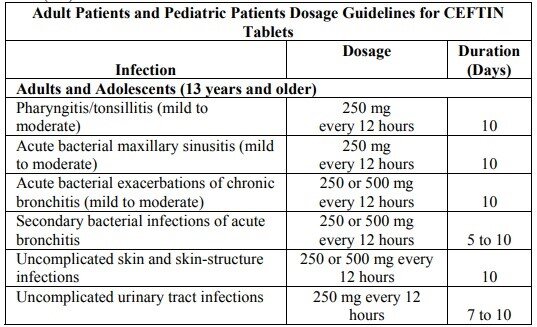 Cr: FDA
Cr: FDA
The dosages listed here are standard, but your doctor may adjust your regimen based on your condition, weight, other diseases, allergies, other medications, and additional factors. Never change a dose without consulting your doctor. Do not start or stop using Ceftin without a prescription.
Finish the full treatment course as advised, even if your symptoms begin to improve. Completing the course helps fully treat the infection and reduce the risk of relapse and antibiotic resistance.
Try not to skip doses or "make up" for a missed dose. If you miss a dose, contact your doctor for advice.
Adult Patients
Adult dosing is generally used for adolescents 12 years and older and adults. Typical doses range from:
- 250 mg twice daily;
- to 500 mg twice daily.
Usually, the course lasts 7 to 10 days, but your doctor may change the duration depending on your specific case.
For best absorption, take the tablets with meals. Do not crush the tablets; swallow them whole with a full glass of water. If possible, do not split, chew, or crush the tablets.
Pediatric Patients
Pediatric patients are usually prescribed the oral suspension form of Ceftin (see below).
Ceftin Dosage for Oral Suspension
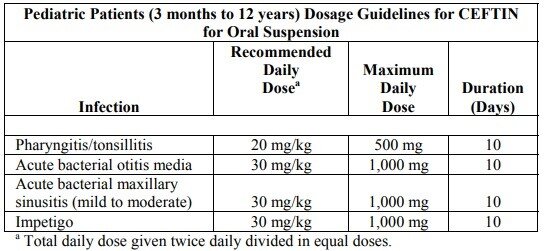 Cr: FDA
Cr: FDA
Pediatric Patients (3 Months to 12 Years)
Pediatric patients are children younger than 12 years. Dosing depends primarily on body weight:
- 10 mg/kg twice daily;
- 15 mg/kg twice daily.
The course also typically lasts 7 to 10 days but may be changed by the doctor. The final dose depends on the condition being treated.
Oral syringes can be used to measure the dose more accurately. You can also use teaspoons, but a syringe is more reliable when precise dosing is required.
Missing a Dose
If you miss a dose, take it as soon as you remember. However, if it is almost time for your next dose, skip the missed dose. Do not take a double dose to make up for a missed one, as this may cause an overdose.
Ceftin Overdose
If you accidentally take too much Ceftin, call emergency services immediately or contact the Poison Help hotline at 1-800-222-1222. If you feel like you may have a seizure, ask someone nearby for help.
Overdose can be accompanied by seizures, convulsions, or blackouts.
Cefuroxime Side Effects
Cefuroxime has a list of possible side effects. Some require urgent medical attention, while others can be discussed at your next appointment. Common side effects of Ceftin include:
- Diarrhea;
- Nausea;
- Vomiting;
- Diaper rash in infants;
- Change in taste.
Tell your doctor if you have any of these side effects. If they don't go away, you may need a change in dose or treatment.
Also, keep in mind that the effects listed in the prescribing information are not a complete list. There may be other individual effects you should discuss with your doctor. If you experience any unusual issues connected to the use of Ceftin, you can also report them to the FDA at 1-800-FDA-1088.
Requiring Immediate Medical Attention
Side effects requiring immediate medical help include:
- Allergic reactions such as difficulty breathing, swelling, or hives;
- Severe stomach pain;
- Watery or bloody diarrhea;
- Severe skin rash;
- Easy bruising;
- Numbness;
- Severe tingling;
- Yellowing of the eyes and/or skin;
- Seizure;
- Signs of kidney problems (urination changes, severe swelling in the feet, fatigue, shortness of breath);
- High fever;
- Burning in the eyes;
- Skin pain, blistering, or peeling.
If symptoms are severe, painful, or rapidly worsening, seek medical attention as soon as possible.
Pregnancy or Breastfeeding Warnings
Tell your doctor if you're pregnant, planning to become pregnant, or breastfeeding. While there are no proven cases of harm to an unborn baby, your doctor may adjust the dose or schedule of your treatment.
Cefuroxime passes into breast milk and may cause allergic or other reactions in the nursing infant.
Keep in mind that cefuroxime may make hormonal birth control less effective. Talk with your doctor about whether you should use additional contraception.
Cefuroxime is not recommended for children younger than 3 months old unless clearly needed.
What Will Affect Ceftin: Interactions
Cefuroxime interactions are common, which is why you must tell your doctor about your diet, medications, and medical conditions. More on that below.
Alcohol/Food Interactions
It's recommended to take Ceftin tablets with meals. Bioavailability increases by almost 20% when a dose is taken with food. However, bacteriologic response is similar whether the tablets are taken with or without food.
There is insufficient information about whether food improves absorption of the oral suspension.
As for cefuroxime axetil and alcohol, there are no strict warnings that alcohol disrupts absorption, excretion, or efficacy. However, if you experience side effects such as gastrointestinal upset or headache, alcohol may worsen them.
Disease Interactions
The medicine may interact with the following conditions:
- Colitis;
- Renal dysfunction;
- Liver disease;
- Seizure disorders;
- Ferricyanide tests.
Tell your doctor about any of these conditions before starting treatment. These conditions may increase the risk of medication buildup and side effects.
Medicine Interactions
Cefuroxime interactions may include:
- Aminoglycoside antibiotics (amikacin, gentamicin, tobramycin, etc.);
- H2-receptor antagonists (famotidine, ranitidine, etc.);
- Antacids (aluminum hydroxide, calcium carbonate, magnesium hydroxide, etc.);
- Hormonal birth control;
- Bacillus Calmette-Guérin (BCG);
- Disulfiram;
- Sodium picosulfate.
It may also interact with the following vaccines:
- BCG vaccine;
- Cholera vaccine;
- Typhoid vaccine.
Review your prescriptions and tell your doctor if you take any of the medicines listed above before, during, or after a course of Ceftin. Depending on your situation, your doctor may adjust doses or timing.
Keep in mind that an interaction does not always mean you must stop a medicine. The decision depends on your condition, severity, side effects, and other factors.
The medications listed above are not the only ones that may interact with Ceftin. If you take any other medicines, make sure your doctor knows about them. If you notice any changes in your condition, contact your doctor promptly.
If you frequently drink alcohol or coffee or smoke cigarettes, mention it during your appointment.
Blood thinners, anti-diarrhea medicines, and other drugs may interact with antibiotics as well, so don't take them without medical advice.
Storage and Handling
Proper storage and handling are important for the medicine's effectiveness. Here are some general recommendations for storing, handling, and disposing of Ceftin:
- Read the label and prescribing information carefully and follow all directions;
- Don't take the medicine in a larger or smaller amount than prescribed;
- To reduce stomach upset, do not crush or chew the tablets;
- Shake the suspension well before measuring a dose;
- Refrigerate the suspension at 36-46°F (2-8°C);
- Discard the suspension if not used within 10 days;
- If switching dosage forms during treatment, ask your pharmacist about correct dosing;
- Don't stop treatment unless your healthcare provider instructs you to;
- Don't use Ceftin to treat viral infections; see a healthcare provider for proper diagnosis and treatment;
- If you're having urine testing, be aware that some tests may be affected;
- Store tablets at room temperature in a dry, cool place;
- Keep the container tightly closed when not in use;
- Do not freeze the suspension;
- Keep all forms of Ceftin out of reach of children and pets;
- Do not dispose of medicines by flushing them or pouring them down a drain, unless instructed to do so.
For disposal recommendations, ask your pharmacist or follow local guidance. If no take-back program is available, you can mix tablets or suspension with an undesirable substance (e.g., cat litter, dirt, or used coffee grounds), place the mixture in a sealed bag or container, and dispose of it in household trash.